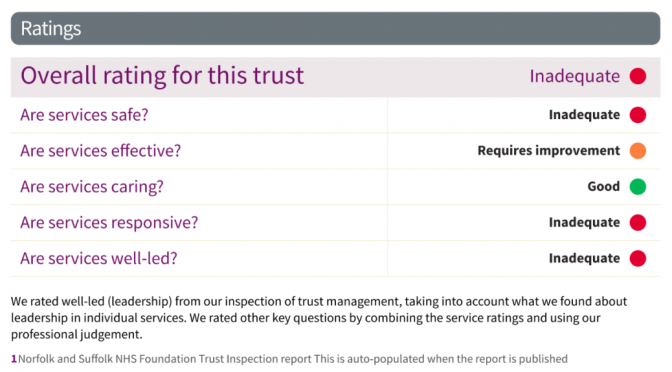
“Inadequate” is such an insipid inadequate term to describe an abject failure to manage critical mental health services and to continue over 5-years to fail to improve.
Norfolk & Suffolk NHS Foundation Trust is the seventh largest mental health trust in the UK, running over 100 community
services across 50 sites and GP practices for 1.6 million people in an area of 3,500 square miles for £227m a year. In any one month they may have 25,000 patients being seen or served. No small feat.
I’ve had great NHS care and compassion, supported by superb individuals via NSFT, Wellbeing, CMHT, Therapy services within Norfolk Mental Health – indeed CQC scored it “Good” for caring. However, the waiting lists for many are criminally irresponsible. This isn’t even my usual rant about transgender waiting lists, although they form a part of mental health. The Government austerity cuts and CCG and NSFT financial and provision managers are presumably to blame as every other trust must be facing similar challenges. Mental Health services remain grossly underfunded and in crisis. Parity for mental health services with physical health and its 18-week guarantees are years away. NSFT tops the table in the worst possible way, making national news today. Norwich topping the football – great; NSFT topping the worst mental health care trust for 5 years – fail!
“NSFT doctors first raised concerns over cuts in January 2013, as more than 500 mental health jobs faced the axe in what was known as a radical redesign of services. Senior psychiatrists warned at the time that patient safety would be put at risk and said the trust was being “downright dishonest’’ for failing to state that the cuts would have detrimental effects on patient care.” – EDP
I had to fight for well over a year to get seen, assessed (I was “lost” in the system three times but with zero response to internal complaints raised), and keep my care – which I am losing in 3 months – apparently, long-term mental health symptoms can be in “recovery” (mine can be episodically), and bipolar and anxiety disorder be signed-off.
“36 people had waited five years to be seen and 2,732 were waiting for their first contact with services… 2,400 adult patients across the trust had not been allocated a care coordinator in community mental health services.” – EDP
This is the problem when capitalist market budgeting is applied to health, and recovery models applied to long-term ailments. I prefer a “discovery” model that supports but doesn’t focus on discharge until you yourself know you are ready. Instead, a benefits and unemployment model of punishing mental health as if it was an aspect of an alleged “work-shy” culture leads to shaming those in need of its services and a seemingly deliberate or incompetent policy of actually signposting ease of access to services resulting in many people never even finding the door, let alone making it through it. Whilst I am currently being “shown the door“, having had an exit strategy meeting, others are shown the door but not let in. As many friends of mine know all to well, just as with PIP applications and appeals, if you weren’t ill when you asked for help by the time you eventually get it the very wait will have made you ill, and certainly resulted in a deterioration of any conditions you have.
“The Care Quality Commission found patients desperately needing care were waiting so long for help they harmed themselves or took overdoses during delays – or were being turned away completely…Staff were covering up the length of waiting lists by allocating patients to staff or running several lists whilst agreeing that nothing would be offered until space was available. And some patients had been waiting five years for help.” – EDP
During a suicidal day, several years ago, I rang the 24hr acute line at Hellesdon on a Friday night and got a locum of some form who said: “I can’t help you, I can’t access your notes at a weekend” and was generally unintelligible and useless in several other ways. I never rang them again.
With a history of suicide, I’ve learned to stay alive by building my own care package and it includes my partner, friends, Wellbeing, CMHT – the “severe and enduring mental health needs” service (keeps getting renamed!), cats, honesty, whisky, and avoiding pills as an accessible suicide kit.
I have nothing but praise for 95% of the frontline staff who’ve helped me. I would not have survived continuing mental health challenges and rebuilt some of my life had it not been for my care team who have gone above and beyond their job descriptions to support my whole wellbeing and not just my mental health. That has included helping me with referrals to physio and general health, and applying for Housing Benefit, PIP and ESA for me, when I was in no state to do so. They are my heroes. The system of cuts and carelessness elsewhere that meant I needed them has probably meant that others have had less support or are still waiting.
“We want services which are provided for those who most need care. That may mean those who don’t have as much need wait a little longer.” – Antek Lejk, Chief Exec NSFT, EADT
Clearly, they are people that carry on caring despite the system and resources they are forced to work with. It is a wonder why so many keep working and don’t leave. Indeed, NSFT has 1-in-4 unfilled nursing posts.
“A perfect storm of cuts, incompetence and stigma has seen services unravel, with people struggling to access services, being discharged too soon, and staff under intolerable pressure with unmanageable caseloads. Following a savage real-terms budget cut, the number of doctors has been reduced by 51 (around 25pc) and the number of nurses by 163 (1 in 8) compared to when the trust was formed in 2012, while referrals have rocketed. The number of patients referred but still awaiting their first contact is 2,732 (as of October 12). That’s a lot of people in distress, without support.” Emma Corlett,EDP
When the CQC interviewed me for a previous report, I said that continuity (and accessibility) of care were critical as my care team kept getting changed or staff going off long-term sick themselves (probably stress at work based).
What happened? Three months later they shuffled the deck chairs (a “radical redesign” no doubt) and changed my care-co again, and I’ve had 3 more since. NSFT is that Titanic on which the deck-chairs get regularly rearranged rather than addressing the approaching iceberg of yet more service-users drowning in a cold heartless sea where the lifeboats are knocked-off the list of necessary equipment to save money.
“The key to keeping people safe is a trusting relationship. How can that be possible with repeated, persistent disruption. Worse of all, it’s deliberate disruption as like you describe, inept managers with a lack of a clue about what else to do opt to do another reorganisation, over the heads of staff and in some cases not even bothering to tell the service user.” – Emma Corlett, Nurse and Norfolk Councillor